
This post is part of our series on the National Science Foundation I-Corps Lean LaunchPad class in Life Science and Health Care at UCSF. Doctors, researchers and Principal Investigators in this class got out of the lab and hospital talked to 2,355 customers, tested 947 hypotheses and invalidated 423 of them. The class had 1,145 engagements with instructors and mentors. (We kept track of all this data by instrumenting the teams with LaunchPad Central software.)
- Part 1: issues in the therapeutics drug discovery pipeline
- Part 2: medical devices and digital health
- Part 3: described what we’re going to do about it
- Part 4: This Will Save us Years – Customer Discovery in Medical Devices
- Part 5: Value proposition and customer segments in Life Sciences
- Part 6: Distribution channels in Life Sciences
- Part 7: Revenue Streams in Life Sciences
- Part 8: When Customers Make You Smarter: Customer Discovery in Digital Health
- Part 9: We’ve seen the Future of Translational Medicine and it’s Disruptive
- Part 10: Lessons Learned in Digital Health
- Part 11: Lessons Learned in Medical Devices
- Part 12: Lessons Learned in Therapeutics
- Pierre-Antoine Gourraud – PhD, MPH UCSF neuroscientist and c0-leader of the MS BioScreen project
- Jason Crane – PhD UCSF Manager Scientific Software Development
- Raphaelle Loren – Managing Director – Health Practice at the Innovation Management Institute
Todd Morrill was the diagnostics cohort instructor. Matt Cooper CEO of Carmenta BioSciences was the Mira Medicine team mentor.
Multiple Sclerosis – MS
Multiple Sclerosis – MS – is an immune system disease that attacks the myelin, the fatty sheath that surrounds and protects nerve fibers of the central nervous system (brain, spinal cord, and optic nerve). T-cells, (a type of white blood cell in the immune system,) become sensitized to myelin and cross the blood-brain barrier into the central nervous system (CNS). Once in the CNS, these T-cells injure myelin, and secrete chemicals that damage nerve fibers (axons) and recruit more damaging immune cells to the site of inflammation. 
Mira Medicine and Multiple Sclerosis
The team came to class with the thought of commercializing the UCSF Multiple Sclerosis BioScreen Project a Precision Medicine application that integrates a patients medical records with the latest population-based data from hundreds of other Multiple Sclerosis patients, (including their 3D MRI scans,) and using predictive algorithms makes it possible to chart a unique course of treatment for each patient. (Mira Medicine team member Pierre-Antoine Gourraud was the project co-leader.) 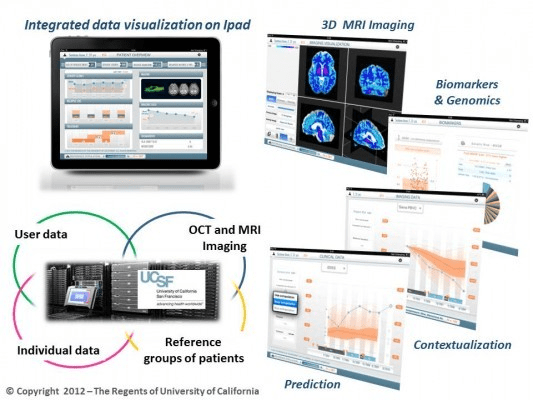
Mira wanted to commercialize the UCSF Multiple Sclerosis Bioscreen project and to add additional neurological diseases which require multiple types of data (including biomarkers, clinical, and imaging). They wanted to help medical centers and large providers assess disease progression to guide therapeutic decision-making. Over the course of the class Mira Medicine team spoke to over 80 customers, partners and payers.
Here’s their 2 minute video summary
If you can’t see the video above, click here.
Then reality hit. First, the team found that their Multiple Sclerosis Bioscreen application (which they used as their MVP) was just a “nice-to-have”, not a “must-have”. In fact, the “must have features” were their future predictive algorithms. Next, they found that if their tool can enable a diagnosis, (even without claiming it could) then it was likely that the FDA would require a 510(k) medical device clearance. Then they found to get reimbursed they need a CPT code (and they had to decide whether to code stack – using multiple codes for “one” diagnosis, and thereby getting multiple reimbursements for one test. (The rules have changed so that code stacking is hard or impossible), Or get a new CPT code, or use miscellaneous code.) To get a new CPT and a 510(k) they would have to perform a some sort of clinical study. At a minimum a 1-year prospective study (a study to see if the neurologists using the application had patients with a better outcome then those who didn’t have access to the app). Getting approval to use an existing (aka old) CPT code means showing equivalence to an existing dx process or test, and the requirements are code-specific. Finally, to get access to data sources of other MS patients they would need to have HIPPA Business Associate Agreement.
Watch their Lessons Learned video below and find out how they pivoted and what happened.
If you can’t see the video above click here
Look at their Lesson Learned slides below If you can’t see the presentation above, click here
Lessons Learned
- Researchers and PI’s come in believing “My science/project/data are so good that people will immediately see the value and be willing to pay for it. It will “sell itself”.
- A business is much more than just good science: it is about customers seeing value and being willing to pay and proper validation and reimbursement coding and…
- A successful business is the sum (and integration!) of all the parts of the business model canvas.
- It includes reimbursement, regulation, IP, validation, channel access, etc.
Listen to the blog post here [audio http://traffic.libsyn.com/albedrio/steveblank_hplewis_140102_FULL.mp3]
Download the podcast here
Share this:

Filed under: Customer Development, Lean LaunchPad, Life Sciences (NIH), NIH (National Institutes of Health), Teaching |
Hey Steve,
As CFO for an emerging Diagnostics company here in Melbourne, Australia I’ve been following progress closely. Be keen to be in touch more with Todd or the group to better understand where they ended up with understanding the ecosystem in terms of payors etc (there was mention in one of Todd’s updte of them updating this every week) as well as lessons learned re: CPT codes. Are you able to pass on my email contact details if they’re open to sharing learnings further directly. Thanks and regards
Remco Marcelis
remco@marcelis.com.au